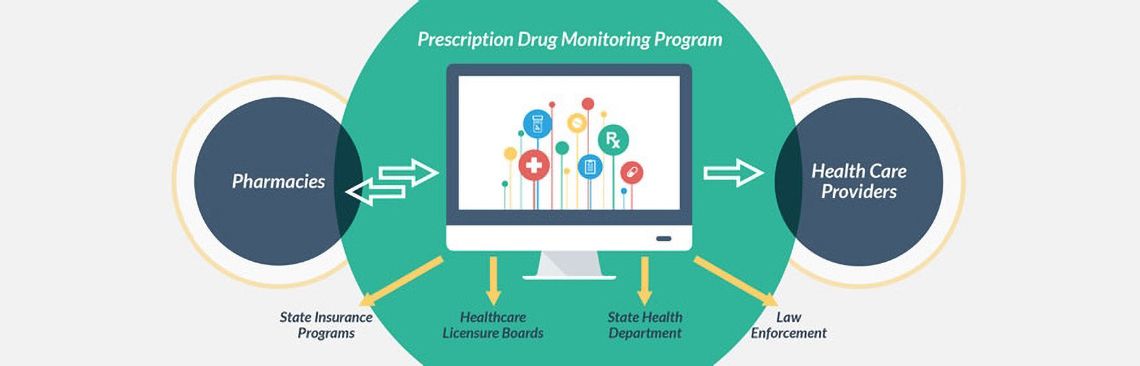
Prescription Drug Monitoring Programs (PDMPs) used in the Emergency Department have been proven to inform and improve opioid prescribing practices in the ED, therefore reducing the number of opioid prescriptions written1. Implemented in 49 states, these databases track Schedule 2-5 controlled medications and generate an individual report for each patient listing all prescriptions written in the past year, including dosage, prescriber, pharmacy, and date prescribed2. This information can help ED physicians to identify opioid misuse, abuse, or diversion. As Emergency Departments physicians ranked 3rd among specialists prescribing the highest number of opioids, the ED is an important setting for PDMPs to be utilized3.
There is ample evidence supporting the effectiveness of PDMPs in improving clinical decision-making for opioid prescribing among ED physicians. A study analyzing ED physician utilization of PDMPs in Wisconsin (n = 63) found that 97% of users reported that it was helpful in identifying patients with patterns of drug abuse and 90% of providers prescribed fewer opioids as a result4. However, 36% of physicians from the sample size did not use the program, with commonly reported barriers being limited knowledge on the registration process or not obtaining a DEA number. A quality improvement project in Pennsylvania aimed to educate ED providers on the use of PDMPs and then measured opioid prescriptions post-education. They found that PDMPs use resulted in a decreased number of opioid prescriptions written5. The cited barriers to usage included issues with access and processing.
Among Maryland physicians, 70% of those using PDMPs reported that the program improved their comfort level when prescribing opioids and decreased the number of opioid prescriptions written, as a cross-sectional survey found (n = 405)6. 74% of these physicians reported PDMP data to be “very useful” in improving their clinical decision-making regarding opioid prescribing. The main barriers to use included limited knowledge on the existence of the program and registration or access difficulties, with 20% of physicians reporting issues with accessing data. Among these cited studies, the most common ones reported barriers to PDMP use include a lack of physician knowledge on the topic and registration issues. In order for PDMPs to yield the most benefit, it is important to address and create solutions for these barriers to use.
These studies substantiate the effectiveness of PDMPs in informing and improving ED provider decision-making around opioid prescribing. The evidence demonstrates that these programs have resulted in fewer opioid prescriptions being written, suggesting that PDMPs may be a useful prevention tool in reducing opioid abuse.
References
-
Elder JW, DePalma G, Pines JM. Optimal Implementation of Prescription Drug Monitoring Programs in the Emergency Department. Us National Library of Medicine, NIH. https://www.ncbi.nlm.nih.gov/pubmed/29560070. Published 2018. Accessed June 21, 2019.
-
Prescription Drug Monitoring Programs: A Guide for Healthcare Providers. Store.samhsa.gov. https://store.samhsa.gov/system/files/sma16-4997.pdf. Published 2017. Accessed June 21, 2019.
-
Lyapustina, T. , Castillo, R. , Omaki, E. , Shields, W. , McDonald, E. , Rothman, R. and Gielen, A. (2017), The Contribution of the Emergency Department To Opioid Pain Reliever Misuse And Diversion: A Critical Review. Pain Pract, 17: 1097-1104. doi:10.1111/papr.12568.
-
Hernandez-Meier J, Muscott R, Zosel A. The Use of a Statewide Prescription Drug Monitoring Program by Emergency Department Physicians. - PubMed - NCBI. Ncbi.nlm.nih.gov. https://www.ncbi.nlm.nih.gov/pubmed/29323819. Published 2017. Accessed June 21, 2019.
-
Martello J, Cassidy B, Mitchell A. Evaluating Emergency Department Opioid Prescribing Behaviors After Education About Mandated Use of the Pennsylvania Prescription Drug Monitoring Programs. - PubMed - NCBI. Ncbi.nlm.nih.gov. https://www.ncbi.nlm.nih.gov/pubmed/30180006. Published 2018. Accessed June 21, 2019.
-
What States Need to Know about PDMPs | Drug Overdose | CDC Injury Center. https://www.cdc.gov/drugoverdose/pdmp/states.html. Published April 29, 2019. Accessed October 10, 2019.

Erica Chemtob is a research fellow for Urgent Matters and a 3rd year Medical Student at the George Washington University School of Medicine & Health Sciences. She received her Bachelor’s Degree in Public Health from the George Washington University and was a Presidential Academic Scholar, a NCAA D1 Student-Athlete on the Varsity Squash Team, and a music minor studying violin. Prior research experience includes the National Institute of Drug Abuse (NIH) and the Washington-Baltimore High Intensity Drug Trafficking Areas Office. She also served as a research assistant for the Center for Advancing Correctional Excellence Lab under Dr. Faye Taxman. She was also a squash coach at Squash On Fire, and performed violin at the Kennedy Center and Carnegie Hall.